 Mitch Keamy is an anesthesiologist in Las Vegas Nevada
Mitch Keamy is an anesthesiologist in Las Vegas Nevada
 Andy Kofke is a Professor of Neuro-anesthesiology and Critical Care at the University of Pennslvania
Andy Kofke is a Professor of Neuro-anesthesiology and Critical Care at the University of Pennslvania
 Mike O'Connor is Professor of Anesthesiology and Critical Care at the University of Chicago
Mike O'Connor is Professor of Anesthesiology and Critical Care at the University of Chicago
 Rob Dean is a cardiac anesthesiologist in Grand Rapids Michigan, with extensive experience in O.R. administration.
Rob Dean is a cardiac anesthesiologist in Grand Rapids Michigan, with extensive experience in O.R. administration.
I am especially interested in the deep hypothermic circulatory arrest used for this because it’s a great example of survivable human brain ischemia. My colleagues in cardiac anesthesia are particularly interested in brain protection during cardiac surgery and I am interested in brain protection in all situations. So I have taken a bit of an interest in this. (Click on all figures to expand)
Some observations:
Here is the number of DHCA cases that my colleagues do annually:

Some pretty good program growth here.
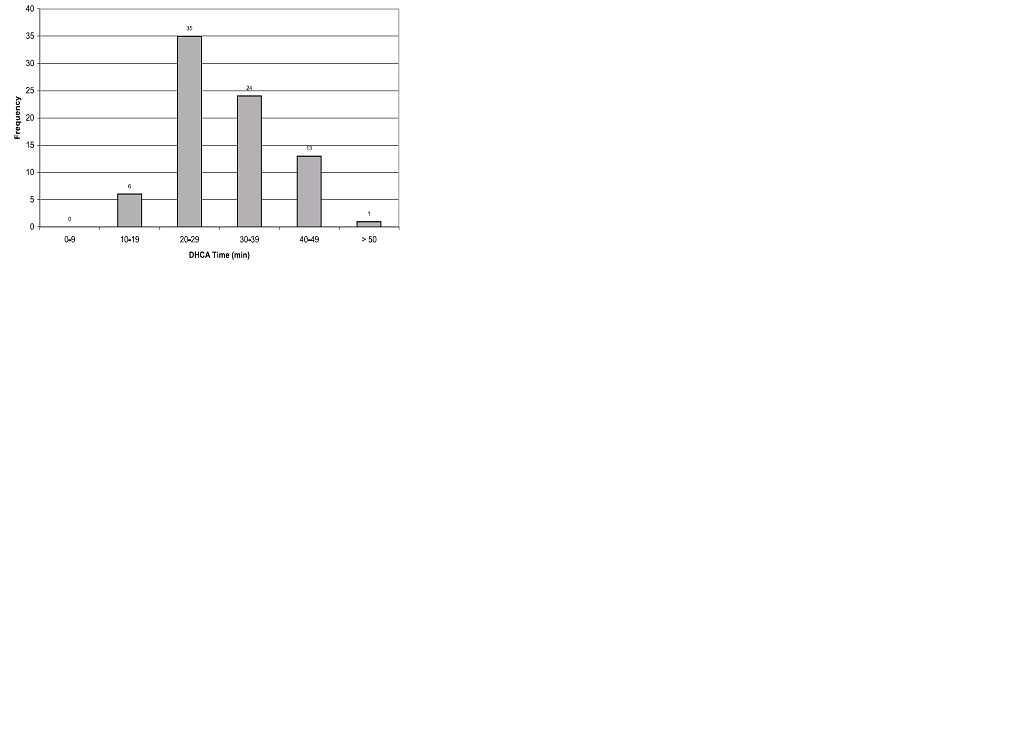
Here is the distribution of
time of DHCA for aortic arch repair. John
Augoustides gave me this figure:

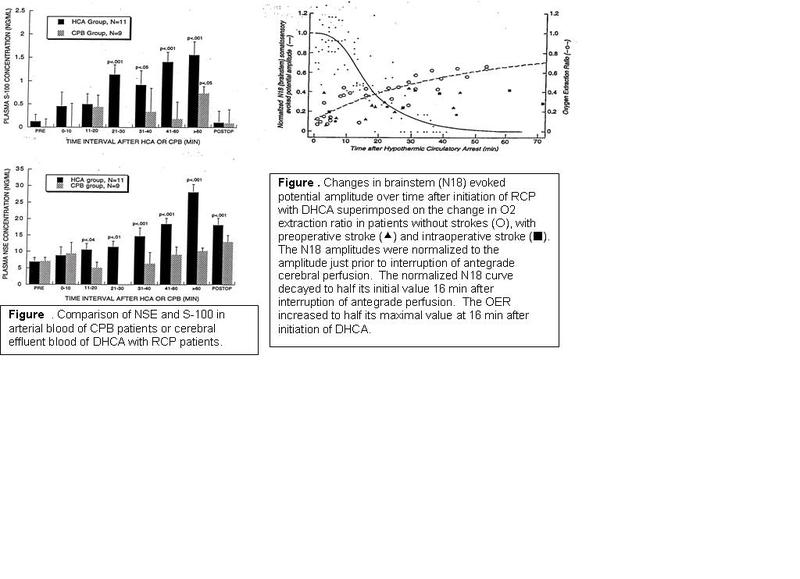
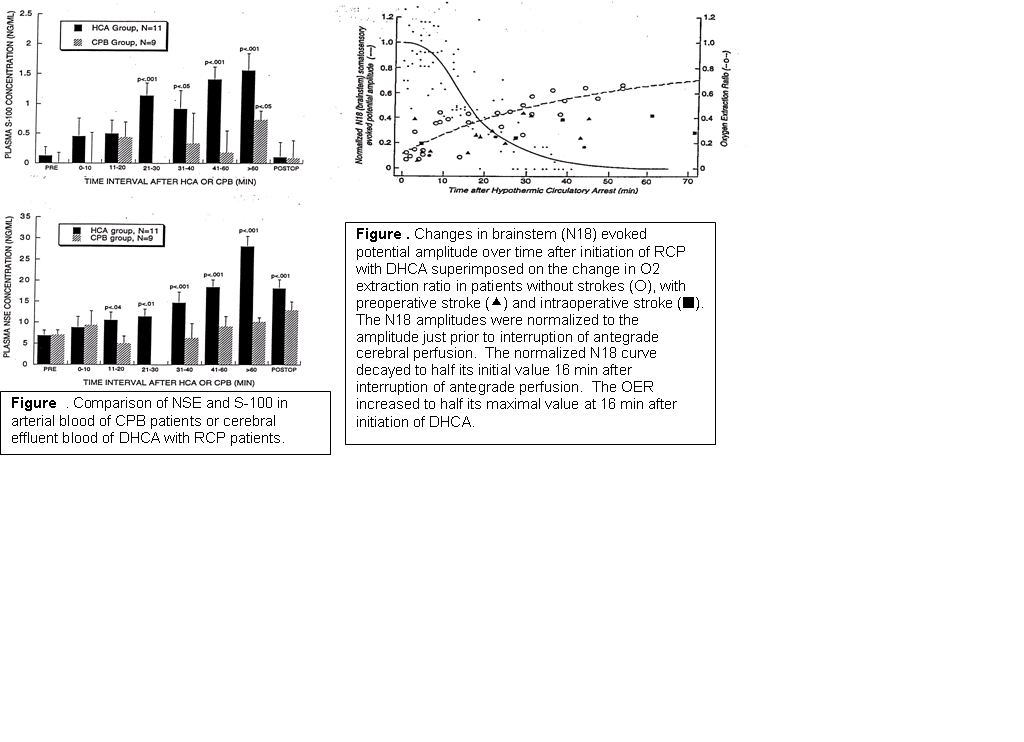
This figure from data collected by Albert Cheung and colleagues suggests that after about a half hour to an hour time’s up:

{kind=link}
{kind=link}
{kind=link}
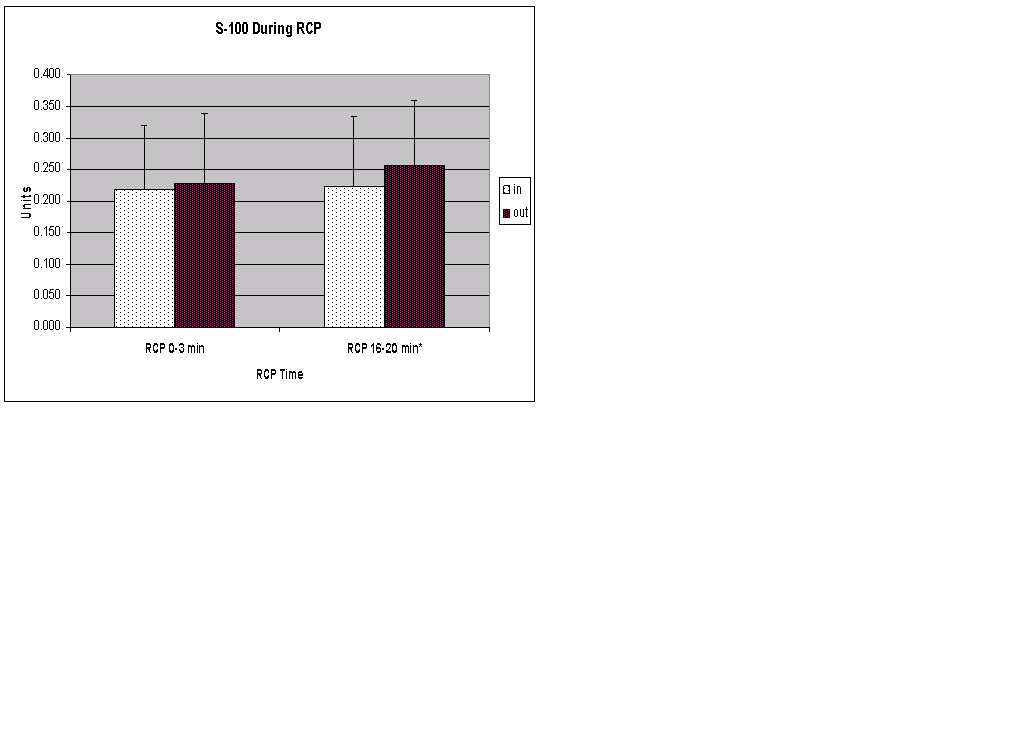
Yes this is interesting but maybe the biomarkers were elevated by the bypass itself. So Hetal Hosalkar, John Augoustides, myself and others organized an effort to compare in vs out suggesting that the brain by 20 minutes of DHCA is putting out S100(* p<.05):

{kind=link}
In regular CABG surgery we were able to show that

the postop release of biomarkers of brain injury varied according to genotype. Here we demonstrate that having the ApoeE4 genotype results in higher levels of S100.
Maybe it makes for worse neuro outcome, but we did not measure that:
Despite the above data, the patients generally do remarkably well
after such a big operation. I worry that
there may be some fairly subtle neurocognitive effects that vary with
genotype. This material is taken from the preliminary
data of a grant I am working on. I am
just dying to know if this model can be used to make generalizable
inferences
about variations in genotypes and their impact on human brain ischemia,
using SNP technology. It is taking so long to get it funded this
may be a literal description (the dying part). Much
of it is already published and can be found by searching on the names
Augoustides,
Kofke, Cheung, and
This is what I’ll look like by the time this stuff gets funded:

This is really good stuff! What is your sense of the value of retrograde flow on duration of protection?
Posted by: mkeamy | September 22, 2024 at 01:29 PM
According to my colleague yianni augoustides:
The Penn practice is to institute DHCA with routine RCP for a maximum duration of 40-45 minutes. If longer DHCA times are required, then typically we employ antegrade cerebral perfusion.
However, this practice varies significantly at high-volume centers around the world.
Posted by: andrew kofke | October 01, 2024 at 01:38 PM
very nice your blog
Posted by: esteban | May 11, 2024 at 06:49 AM
According to my colleague yianni augoustides:
The Penn practice is to institute DHCA with routine RCP for a maximum duration of 40-45 minutes. If longer DHCA times are required, then typically we employ antegrade cerebral perfusion.
However, this practice varies significantly at high-volume centers around the world.
+1
Posted by: flash games collection | July 10, 2024 at 06:33 PM